
Antibiotic resistance is increasing at a rapid rate making pathogens and other bacterial species resistant to currently available antibiotics. Its impact is already visible globally and clock is ticking faster than ever pushing scientists all over the world to develop better antibiotics with higher specificity (only!) for pathogens. Antibiotic consumption is directly related to antibiotic resistance and policies across the continents are underway to control the consumption and prescription of antibiotics.
A recent article in elife introduces the problem of unnecessary antibiotic use and provides data to avert it.
“Inappropriate antibiotic use leads to increased risk of adverse events, disruption of colonization resistance and other benefits of the microbial flora, and bystander selection for antibiotic resistance, with little to no health gains for the patient.”
To address the problem, Christine et al. used publically available data (NAMCS/NHAMCS) and mathematical models to find what would happen if antibiotic consumption is averted in hypothetical scenarios.
What they did?
“The analysis included sixteen antibiotics that are frequently prescribed in the outpatient setting and nine potentially pathogenic bacterial species that are commonly carried in the normal human microbiome. For each antibiotic-species pair, they estimated the proportion of antibiotic exposures experienced by that species that could be averted under four hypothetical scenarios.
1) Eliminate unnecessary antibiotic use across all outpatient conditions.
2) Eliminate all antibiotic use for outpatient respiratory conditions for which antibiotics are not indicated.
3) Eliminate all antibiotic use for acute sinusitis.
4) Prescribe nitrofurantoin* for all cases of cystitis in women.”
“*Nitrofurantoin- a recommended first-line therapy with good potency against common uropathogens, low levels of resistance, and decreased risk of collateral damage to the intestinal microbiome”
Results
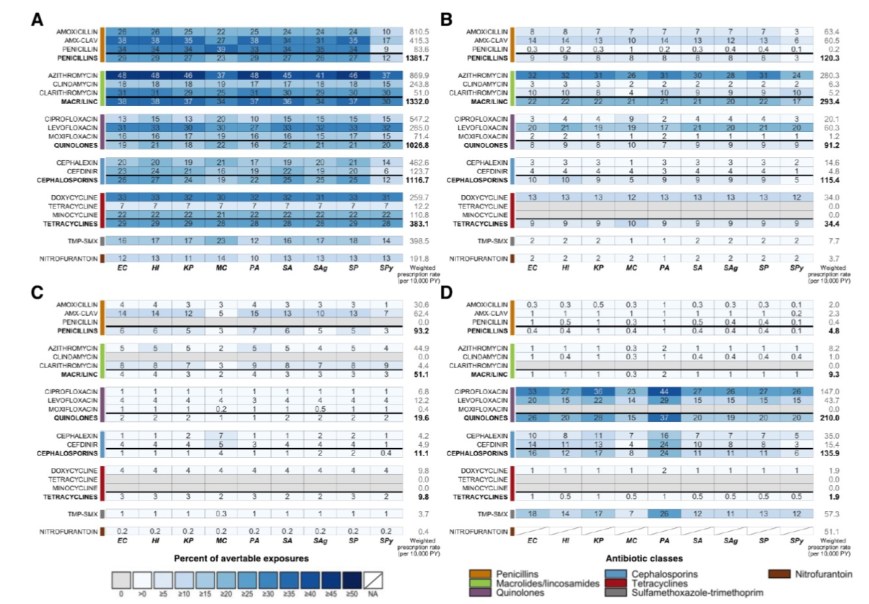
Heatmaps showing the estimated percentage of species exposures to each antibiotic or antibiotic class that could be averted if A: unnecessary antibiotic prescriptions across all outpatient conditions, B: all antibiotic use for outpatient respiratory conditions for which antibiotics are not indicated, C: all antibiotic use for acute sinusitis, or D: non-nitrofurantoin treatment of cystitis in women was eliminated. Drug class results include prescriptions of all antibiotics in that class, as identified by the Lexicon Plus classification system.
Abbreviations: Antibiotics (y-axis): AMX-CLAV=amoxicillin-clavulanate,, MACR/LINC=macrolides/lincosamides, TMP-SMX=sulfamethoxazole-trimethoprim;
Organisms (x-axis): EC=E. coli, HI=H. influenzae, KP=K. pneumoniae, MC=M. catarrhalis, PA=P. aeruginosa, SA=S. aureus, SAg=S. agalactiae, SP=S. pneumoniae, SPy=S. pyogenes; PY=person-years
The darker shades in panel A (scenario 1) clearly indicated that “elimination of unnecessary antibiotic prescriptions across all outpatient conditions would prevent 6 to 48% (IQR: 17 to 31%) of antibiotic-species exposures. If all unnecessary antibiotic use could be prevented, over 30% of exposures to amoxicillin-clavulanate, penicillin, azithromycin, clarithromycin, levofloxacin, and doxycycline across most potential pathogens of interest could be averted.”
In panel D (scenario 4), they found that prescribing nitrofurantoin not only averted antibiotic exposure in non-causative bacterial species (bystanders) but also in causative species for cystitis in women.
“Overall, 27% of ciprofloxacin use is associated with acute cystitis in women. Organisms that are not causative pathogens of cystitis have proportions of avertable exposures close to or less than 27%, but a substantially higher proportion of exposures could be averted among causative pathogens – 33%, 36%, and 44% of ciprofloxacin exposures to E. coli, K. pneumoniae, and P. aeruginosa, respectively.”
The study addresses the limitations with regard to data availability and reporting in public database. Authors are cautious and point out,
“It is important to note that the reduction in antibiotic exposures estimated here does not translate to the same reduction in the prevalence of resistance or in the morbidity and mortality attributable to resistance. Additionally, in this analysis, we give each exposure equal weight. However, the selective pressure imposed by a single exposure depends on a number of variables, including pharmacokinetics, pharmacodynamics, distribution of bacteria across body sites, and bacterial population size. For example, we might expect that the probability of resistance scales with population size, and thus that an exposure received by an individual with higher bacterial load will have a larger impact on resistance.”
Overall, this study indeed provides evidence that “improved prescription of antibiotics has the potential to prevent antibiotic exposure experienced by bacterial species throughout microbiome.”
